 Post-acute care providers are functioning in a world of regulatory acronyms: QAPI, QIS survey, ZPIC, PPS, CERTs, UPICs, ACOs, and more, including programs to improve transitions of care and reduce rehospitalization rates.
Post-acute care providers are functioning in a world of regulatory acronyms: QAPI, QIS survey, ZPIC, PPS, CERTs, UPICs, ACOs, and more, including programs to improve transitions of care and reduce rehospitalization rates.
Operational managers and clinical leadership in nursing homes are evaluating services, training, risks, and outcomes, as well as database content, on a daily basis to monitor outcomes for the elders they serve.
The issue of incontinence management and treatment related to incontinence is central to most of these activities and must be properly identified, treated aggressively, and monitored continuously to eliminate unnecessary cost and negative outcomes. This focus requires participation from operations, clinical staff, therapy, social services, direct caregivers, and families.
Continence Care Must-Haves
The issue of incontinence management is not new at all and has been a frequent topic of discussion for interdisciplinary team members in care conferences, team meetings, and when discussions of risk management and outcomes arise.
The current environment in post-acute care requires a more specific approach and understanding of the definitions in the minimum data set 3.0 (MDS), as well as coordination between related departments, to work to reverse levels of incontinence, when possible, and to minimize the negative outcomes for elders, including rehospitalizations and deterioration in quality of life.
Facilities are now more accountable for the data they transmit on the MDS because of the data references used by state surveyors, policy processes, and payment programs. This is a very expensive and common issue that facilities need to strive to understand, properly manage, and document, especially with regard to the impact of their interventions and programs.
When looking at the definition of continence in the resident assessment instrument (RAI) manual, May 2013 revision, it does not match the working definitions found in the majority of facilities. According to the MDS 3.0, continence is “total control of the release of urine or stool.”
This means that an elder who has stress or effort-related incontinence (urine leakage with a cough or change in position) should be coded as incontinent on the MDS.
The current Centers for Medicare & Medicaid Services (CMS) MDS frequency reports for the first quarter of 2013 show that 23.9 percent of all elders in skilled nursing facilities are totally continent.
This is a statistic that is just simply not true.
A review of F-Tag 315 uses the same definition and then goes on to explain the negative impact that any level of incontinence has on elders in the skilled nursing environment, with a focus on the identification of the type of incontinence, its cause, and treatment. Quality of life and quality of care are the goals, with an individualized approach that is undertaken by the entire team, as well as the family, when possible.
Restorative Program Required
Today, a significant number of facilities do not have active restorative programs that include toileting and retraining. Many have very little coordination between nursing and therapy for bladder and bowel retraining, while some have poor documentation of in-depth quality assessments at the time of admission to determine the true level of continence prior to hospitalization and after-hospitalization.
These are all important factors in the development of an active program to identify and reverse incontinence whenever possible. Elders must also be asked if they want to be continent and have control of their elimination.
According to an 80-year-old resident, newly admitted to a nursing home for rehab after a hip repair surgery, “I know I needed to have my hip repaired, but I did not sign up for this .... [having to wear a brief because of functional incontinence after urinary catheter removal]. I want my rehab to include help with my incontinence.”
The demographics of customers are changing, and the programs need to be there to meet their needs. These are elders who want to go back to their active, positive lives in the community—without incontinence. Nursing centers need to have excellent assessment programs and documentation at the time of admission and be open and interactive about the status of continence.
It is important to initiate retraining or scheduled toileting programs, as well as involving therapy, with strengthening and activities of daily living programs, combined with resident and family education, to support the goals and interventions in the plan.
Assessment Essentials
Careful assessment and identification of the cause(s) of incontinence are the essential first steps for appropriate and successful management. This assessment needs to involve several disciplines, including therapists, nurse practitioners, nurse assistants, nursing staff, medical directors, and dietary staff.
Assessment should be done at the time of admission to the facility and at any change in bladder and bowel status. The first step is determination and documentation of incontinence history on or before the time of admission. Staff should determine the resident’s continence status prior to admission or determine whether it occurred with the present illness, since urinary incontinence (UI) could be of several years’ duration. This requires a conversation with the elder or family members.
Although UI is not a normal part of aging, there are age-related changes in the lower urinary tract, such as that the greatest volume of urine is excreted at night, with two-thirds of daily fluid intake being produced by the kidneys at night. Bladder capacity is diminished with poor bladder emptying, and bladder sensations changes with age, causing a delay in desire to void, leading to bladder frequency.
Mental, functional, and environmental assessments are vital to the success of a restorative program. Cognition should be assessed to determine the ability of the resident to comprehend voiding needs. Knowing when the onset of lower urinary tract symptoms occurred, including urgency, frequency, nocturia, dysuria, post-void dribbling, and episodes of urine leakage, is important. The relationship between UI and medication use and medical diagnoses, such as diabetes, neurologic diseases, such as Parkinson’s or multiple sclerosis; prostate problems in men, such as cancer or benign prostatic hyperplasia; and chronic urinary tract infections, especially in women, should be detailed.
Facility nurses should perform a thorough bowel history of the resident to determine symptoms of constipation, fecal incontinence, and the use of laxatives, stool softeners, suppositories, and enemas. Per the MDS 3.0, an elder’s voiding and bowel pattern and frequency of incontinence should be assessed, so observation of toileting can be helpful.
In addition, nurses should perform a general examination to determine peripheral edema and gait abnormalities that may impact toileting, while an inspection of the genitalia should also be done to determine skin breakdown.
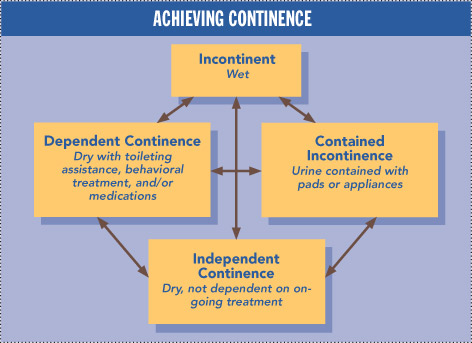
Assessments should lead to a plan of care. The classification of continence, as seen in Figure 1 (see page 63), outlines components of continence management. Centers should have well-defined policies and procedures to initiate and document toileting programs with nursing and therapy.
Determine Staff Knowledge
Facility staff members need to address their knowledge of the topic and develop appropriate documentation skills to identify the type and frequency of incontinence at the point of admission, or before, as part of the key information they need to care for the elder.
Using the appropriate definitions for all staff and transmitting the accurate data into the MDS 3.0 database is the first step to create an accurate facility record.
Reading the facility database reports on the initial levels of continence, followed by subsequent changes in levels of continence as rehab and nursing services improve the resident’s function, gives the manager access to reportable outcomes.
The outcomes of an active continence management program are very easy to identify and document.
If the MDS data are accurate, then tracking levels of success with toileting, ambulation, and balance programs—along with the goal of safely going to the bathroom; getting on and off the commode; control of muscles involved in elimination; and improved dignity, strength, and function—should be straightforward.
Changes in ADL (activities of daily living) scores and symptoms of depression, as well as reduced rates of falls, can all be outcomes that are reportable and desirable in the data-driven world providers work in today. More independence decreases the stress on staff and lessens product use or the type and cost of products.
With regard to payment in case-mix states, restorative programs have a positive impact on Medicaid rates and support Part A rates with the use of the low rehab category after high- intensity rehab is completed.
Incontinence Products
Nursing homes need to evaluate their current products and the variety of sizes and types of products they use. It is essential to have incontinence products that are properly sized, with a variety of types available as the retraining program progresses.
Staff education and training is also essential to delivering toileting programs, documenting outcomes, and elders’ responses. A toileting or retraining program should never be done to an elder, it should be done with the elder.
Scheduled toileting programs can be designed and delivered for elders with memory loss to diminish the number of incontinent episodes and develop a habit of voiding that matches the elder’s intake and activity patterns.
Proper reporting and documentation should include the outcome of a toileting program and the types and sizes of products used so that the care is consistent and connects with the plan. This will have a positive impact on survey outcomes.
Remember, the goal here is increased quality of care and quality of life for the elder, as well as a reduction of risk of falls, behavioral outbursts, moisture-associated skin damage, skin breakdown, and dignity issues.
How To Get Started
It’s a good idea to begin with the CMS definitions and the staff’s knowledge base about continence and incontinence. Use the RAI Manual May 2013 definitions and the October 2013 updates. Assess bladder control issues at the point of admission, and inquire about the level of continence prior to taking a resident to the hospital. Focus on an accurate three-day voiding diary, and build toileting programs from that documentation. Involve the resident and family when appropriate, remembering that it is a matter of involving the resident with the program and not forcing it upon them.
Develop policies and processes for toileting programs, and include education for all clinical staff so programs can be delivered on all shifts with accurate documentation. Include the toileting program and need for muscle strength and retraining with rehab services. Analyze the data, and know what the database says about the issues and outcomes. Look for cost savings, improved outcomes, and increased customer satisfaction.
Leah Klusch RN, BSN, FACHCA, executive director, the Alliance Training Center, Alliance, Ohio, can be reached at leahklusch@sbcglobal.net. Diane Newman, DNP, ANP-BC, FAAN, co-director of the Penn Center for Continence and Pelvic Health, can be reached at diane.newman@uph5.upenn.edu.